I have a friend who spent a decade working customs at an airport, and she used to tell me that the same suitcase could be treated three completely different ways depending on which door it came through. Same contents. Same owner. Three sets of rules, because the rules were never really about the suitcase. They were about the channel.
I keep thinking about her every time someone asks me, flatly, “is tesamorelin legal?” It is a fair question asked the wrong way, because it assumes one answer exists. It doesn’t. Tesamorelin, a single peptide, currently occupies three separate legal positions at once, and which one applies to you depends entirely on the door you walked through to get it. That is not a loophole. It is just how the regulatory architecture happens to be built around this particular molecule. Get the channel wrong in your head, and you will take a true sentence about one door and drag it, mistakenly, through another.
A note before we go further, in the interest of not pretending to be something I’m not: I am a writer, not a physician, and this piece is an explainer, not medical advice. It draws only on primary sources you can open yourself. Tesamorelin is an FDA-approved finished drug, sold as Egrifta, for one narrow use. The body-composition and anti-aging uses it gets marketed for beyond that are off-label. Last checked against the sources in June 2026.
The scorecard, before the story
Before I walk through each door separately, here is the whole map at once. Treat it as a map, not a recommendation.
| Channel | Legal to obtain? | FDA-approved finished drug? | Reviewed for identity/purity? | Approximate monthly cost | Allowed in tested sport? |
|---|---|---|---|---|---|
| Brand Egrifta (Rx) | Yes, with a prescription | Yes | Yes | ~$3,000 to $6,000 | No |
| Compounded (Rx, licensed pharmacy) | Yes, with a prescription | No | Not as a finished product | A fraction of brand | No |
| Research-chemical vial | Legally gray for human use | No | No | Cheapest of the three | No |
Notice something about the rightmost column first, because it’s the easiest to misread. It says “No” three times, and that column never changes no matter which door you walked through. The columns that actually move, the ones worth your attention, are legality of obtaining it, FDA status, and whether anyone has verified what’s actually in the vial. Those three are the whole game.
Door one: the brand, fully legal and priced accordingly
The cleanest door is also the most expensive one. Egrifta is an FDA-approved prescription drug, full stop. The agency approved tesamorelin in November 2010 for reducing excess abdominal fat in HIV-infected patients with lipodystrophy, and the label is a public document laying out that indication, the 2 mg daily subcutaneous dose, and instructions to monitor glucose [R5]. Bought through a prescription, dispensed by a pharmacy, this is as legitimate as medicine gets. There’s no asterisk on its legality.
The asterisk shows up on the receipt. Without insurance, the brand can run somewhere between $3,000 and $6,000 a month, and that single figure explains almost everything else in this article. If Egrifta were priced like a generic, most of the questions people ask me about compounding and research vials would simply not exist. It isn’t, so they do.
Door two: compounded, legal, and a narrower claim than people assume
This is the door where I see the most confusion, because two adjacent-sounding sentences get quietly merged into one.
Sentence one: compounded tesamorelin is legal to obtain, through a licensed compounding pharmacy, with a valid prescription, under physician supervision. True. The supervised telehealth providers operating in this space stand on exactly that ground.
Sentence two: compounded tesamorelin is not an FDA-approved finished drug. Also true, and it does not contradict sentence one. This is where I want to slow down, because a lot of marketing copy relies on readers not noticing the gap between “legal with a prescription” and “FDA-approved.” They are different claims. Compounding operates under a different regulatory framework than finished-drug approval, and that’s not a loophole anyone is exploiting quietly, it’s just what compounding is.
What the gap buys you is price. The compounded route runs at a fraction of the brand’s cost, which is the entire reason it exists as a real option for people who cannot write a $4,000 check every month. What you’re trading is the FDA’s finished-product review. A supervised provider tries to put some of that back: a clinician who screens you, a prescription issued when it’s appropriate, a licensed pharmacy doing the actual compounding, and someone checking in afterward.
Door three: the research vial, and a label doing more work than it looks like
The third door is where the law gets genuinely uncomfortable, and the honest word for it is gray, not green and not red.
A research-chemical seller can market tesamorelin as a laboratory chemical, stamped “for research use only” or “not for human consumption.” That phrase is not legal decoration. Selling a chemical for laboratory research sits in a different regulatory bucket than selling a drug meant to go into a person’s body, and the instant a product is marketed for human use, it becomes an unapproved new drug. The disclaimer exists precisely to keep the sale on the legal side of that line, and it does that job by telling you, in writing, that the product is not meant for you.
So here’s the honest way to score it. You can probably buy the vial. Using it the way you actually intend, by injecting it, is the very use the seller has disclaimed on the label. No prescription touched it. No pharmacy filled it. Nobody checked the identity, strength, or purity of what’s floating in that liquid.
There’s a specific trap in this door that I think distorts people’s math, and it’s worth naming. Because tesamorelin really is an FDA-approved drug with real Phase 3 data behind it [R1][R2], a research vial gets to borrow some of that legitimacy just by sharing a name. The reasoning goes something like: it’s approved, the trials are real, so a vial of it must be basically fine. That’s a quiet swap of two different things. The approval and the trial results describe a pharmacy-dispensed product used under medical supervision. They say nothing about the powder in an unlabeled bottle from a chemical retailer.
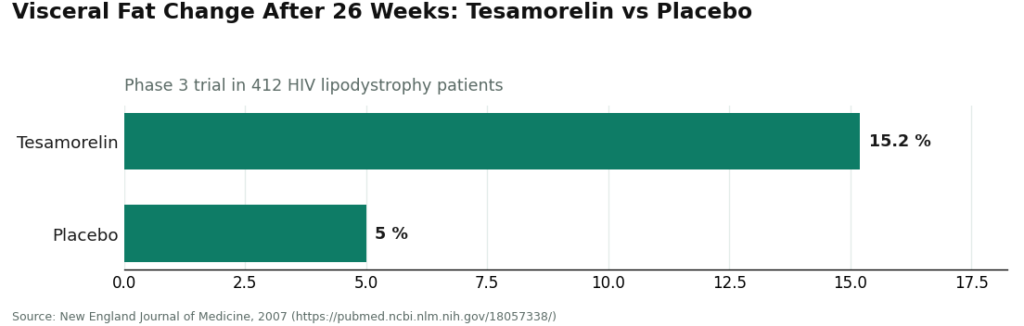
Look at what the actual trial found, because the specificity matters here. In the 26-week Phase 3 study behind that approval, 412 HIV patients on tesamorelin saw visceral fat drop by 15.2%, against a 5.0% increase in the placebo group [R1]. That is real data, describing a real, verified, pharmacy-grade product used under a doctor’s care. It tells you almost nothing about what’s actually in the vial sitting on someone’s kitchen counter, ordered from a website with a disclaimer buried at the bottom of the page. The gap between those two things is the entire risk of door three, and no amount of citing the real trial closes it.
The door that overrides the other three
There’s a fourth layer sitting on top of all this, and it doesn’t care which door you walked through. Tesamorelin appears by name on the WADA 2026 Prohibited List, under category S2, as a growth-hormone-releasing hormone analogue [R6]. Every row in that scorecard reads “No” in the sport column, and that’s not an oversight, it’s the point. A prohibited substance stays prohibited no matter how cleanly you obtained it.
This is, honestly, the tidiest fact in the whole piece. Brand prescription, compounded prescription, research vial, it makes no difference to a drug-testing panel. A “research use only” sticker offers zero cover. A legitimate prescription from a real doctor offers zero cover. If you compete in a tested sport, this molecule is off the table, and since WADA reissues its list every year, check the current version yourself before you go near any peptide [R6].
Where the misreading happens
The most common mistake I see is lifting a true sentence out of one row and setting it down in another. “Tesamorelin is FDA-approved” is true, but only in the brand row, and only for one HIV-related indication. “Tesamorelin is legal with a prescription” holds for the brand and the compounded route, not for a research vial injected into a human body. “Tesamorelin is banned in sport” is the one sentence that travels cleanly across every row. The whole reason to lay this out as a grid rather than a paragraph is that the answer shifts column by column. You can’t flatten it into a single yes or no without losing something true.
A second, quieter mistake is treating legality, FDA status, and safety as though they were the same measurement. They aren’t. Something can be legal to obtain and still not be an FDA-approved finished product, which is exactly the compounded row. Something can be FDA-approved for one narrow use and prescribed off-label for a completely different one, which describes nearly everyone taking tesamorelin for body composition rather than HIV lipodystrophy. Sellers tend to blur these three axes together, deliberately, because “FDA-approved” sounds reassuring in a way that quietly answers a safety question it was never actually asking.
What supervision actually buys you
None of this legal mapping expands the evidence for off-label tesamorelin use. Supervision doesn’t turn an anti-aging application into a proven one. What changes, door to door, is who is accountable if something goes wrong. In the brand and compounded rows, a licensed clinician and a licensed pharmacy sit inside the transaction with you. In the research-vial row, neither one does.
FormBlends is one example of the supervised model, structurally: a physician evaluates you, writes a prescription when it’s appropriate, and a licensed compounding pharmacy fills it, rather than a chemical warehouse shipping a vial with a disclaimer attached. I’m naming it here as an illustration of that middle row on the scorecard, not as an endorsement to buy anything, there’s nothing for sale in this piece. The reason it sits in a different legal position from the research vial isn’t a branding choice. It’s that a clinician and a pharmacy are actually inside the chain, which is the exact distinction the scorecard is trying to measure.
The bottom line, scored honestly
Tesamorelin, in 2026, is legal as a brand prescription, legal as a compounded prescription, and legally gray as a research chemical used in a human body. It is an FDA-approved finished drug only through the brand, and only for HIV-associated lipodystrophy, nothing broader. It is banned in tested sport across every single door, without exception. Price runs from a few hundred dollars compounded up to several thousand for the brand, and the research vial undercuts both because no one is accountable for what’s actually inside it.
If you take one thing from all this, let it be that the answer depends on which column you’re reading. One molecule, three legal statuses, and a sport ban sitting on top that erases the difference between all of them. Read the scorecard by column, not by molecule, and the confusion mostly disappears.
A few questions people keep asking me
Is tesamorelin legal to buy in 2026? It depends entirely on the door. Egrifta, the brand, is fully legal with a prescription. Compounded tesamorelin is legal through a licensed compounding pharmacy under physician supervision, with a valid prescription. A research-chemical vial sits in a legal gray zone for human use, sold “for research use only,” and it becomes an unapproved new drug the moment someone markets it for injection. There’s no single yes or no here, which is really the entire point of laying it out as a scorecard.
Is tesamorelin actually FDA-approved? Yes, but narrowly. The FDA approved it in November 2010, as Egrifta, for reducing excess abdominal fat in HIV-infected patients with lipodystrophy. Compounded tesamorelin is legal to obtain but isn’t an FDA-approved finished product, and the research vial isn’t approved at all. The body-composition and anti-aging uses most people are actually chasing are off-label everywhere.
Why is compounded tesamorelin so much cheaper than the brand? The brand can cost roughly $3,000 to $6,000 a month without insurance. Compounded runs at a fraction of that. What you give up for the lower price is the FDA’s finished-product review, which a supervised provider partially offsets by keeping a licensed clinician and pharmacy inside the transaction.
Can I use tesamorelin if I compete in a tested sport? No, in every case. Tesamorelin is named explicitly on the WADA 2026 Prohibited List, category S2, as a growth-hormone-releasing hormone analogue, and that ban applies regardless of which door you got it through. A prescription offers no protection, and neither does a “research use only” label. WADA updates the list yearly, so check the current version before going near any peptide.
Does a “research use only” sticker make injecting a tesamorelin vial safe or legal? No. That label is doing legal work, not safety work. It keeps the sale in the laboratory-chemical category by declaring the product isn’t meant for human use, which means injecting it is precisely the use the seller disclaimed. Nothing about it has been prescribed, dispensed by a pharmacy, or checked by the FDA for identity, strength, or purity.
What does going through a supervised provider actually change? It doesn’t expand the evidence for off-label use. It changes who’s accountable in the transaction. A clinician evaluates you first, a prescription gets written when it’s warranted, and a licensed compounding pharmacy fills it. FormBlends operates on that model, which puts it in a different legal position from a research vial, where neither a clinician nor a pharmacy is anywhere in the chain.
What is tesamorelin, and how does it actually work?
Tesamorelin is a synthetic peptide built to mimic growth hormone-releasing hormone, the signal your hypothalamus sends telling the pituitary gland to release growth hormone. That downstream release is where the effect comes from. It doesn’t hand your body growth hormone directly, it asks your own pituitary to make more of it, which is a real distinction from injecting synthetic HGH itself.
Does the FDA approval cover general use?
It covers one specific thing: reducing excess abdominal fat in HIV-positive adults with lipodystrophy, approved in 2010 under the name Egrifta. It doesn’t extend to anti-aging, body composition in otherwise healthy people, or anything else. Using or prescribing it outside that narrow indication sits in a different legal and medical category, and that difference shapes how you should think about where you source it.
Do I need to be asleep for it to work?
No, tesamorelin doesn’t require sleep to function. But natural growth hormone release peaks during deep sleep, and the peptide operates inside that same system, so bad sleep can blunt total growth hormone output no matter what’s in the syringe. Most protocols call for an evening dose to roughly track that natural rhythm, but the peptide itself isn’t sleep-dependent.
What are the realistic safety concerns in 2026?
The clearest safety picture comes from clinical trials in HIV lipodystrophy patients, where the common issues were injection-site reactions, fluid retention, joint discomfort, and short-term blood sugar shifts. Long-term data outside that specific population is thin. Anyone with active cancer, a history of pituitary tumors, or poorly controlled diabetes carries more risk. Sourcing through a physician-supervised compounding pharmacy such as FormBlends, rather than a gray-market research vendor, at least puts pharmaceutical-grade purity and medical oversight back into the picture.
References
- Tesamorelin reduced visceral adipose tissue by 15.2% (vs a 5.0% increase on placebo), lowered triglycerides by about 50 mg/dL, and raised IGF-1 by about 81% in a 26-week Phase 3 trial of 412 HIV patients. New England Journal of Medicine, 2007. https://pubmed.ncbi.nlm.nih.gov/18057338/
- Pooled analysis of two Phase 3 tesamorelin trials (806 HIV patients); visceral-fat reduction and lipid improvements maintained to 52 weeks. Journal of Clinical Endocrinology and Metabolism, 2010. https://pubmed.ncbi.nlm.nih.gov/20554713/
- FDA-approved Egrifta (tesamorelin) prescribing information: indicated for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy; 2 mg subcutaneous once daily; monitor for changes in glucose metabolism; long-term cardiovascular safety not established; not indicated for weight loss. U.S. Food and Drug Administration label (original 2010 approval).
- WADA 2026 Prohibited List: growth-hormone-releasing hormone analogues, including tesamorelin, are prohibited in sport under category S2. World Anti-Doping Agency, in force January 2026.